Feedback on the UDOH “Immunization Education Module,” and Surrounding Discussion
Submitted to the Utah Legislature Health and Human Services Interim Committee and Utah Department of Health by Kristen S. Chevrier, MA, on behalf of parents across the state and the Utah Eagle Forum. 10/17/2018
Recent Updates to Immunization Education Module made by UDOH
We went over the updates that were provided by UDOH. Links are not live in the pdf, so we searched for them manually. Even with the new information, the module is misleading, incomplete, and inaccurate. We have provided each committee member with an email version of this document, so that you can peruse linked information as you desire.
Update Link (Provided by UDOH)
In this document, we touch on some of our concerns with the “Immunization Education Module.” Feedback given here follows the order of the presentation. We have not addressed every issue, or addressed any issue in complete detail. We have not addressed slides that appear accurate. We have not seen every module response to every “wrong” answer, and cannot respond to what we have not seen. (We requested actual slides, but were given a link to do the module instead, and took screen shots as we went through, so we could examine the data without having to retake the module multiple times.)
Correction to Statement made in the July HHS Interim Committee Meeting
Dr. Joe Miner: “Only 12 states offer personal and religious exemptions.”
Fact: At least 17 states offer personal exemptions, and 35 offer religious exemptions, with overlap.
Corrections to Statements in the “Immunization Education Module”
“What are vaccines? ‘…more natural than…vitamin supplements.’”
This is stated as fact, with no sources offered. The statement is both misleading and irrelevant. Please see the Vaccine Excipient & Media Summary, linked below. Many substances in vaccines are not recognized by the body as “natural,” or “more natural than vitamin supplements.” The fact that something is a naturally occurring substance does not mean it belongs in the human body. Arsenic is natural; mercury is natural, as are monkey kidney cells, but they are not naturally found in humans or beneficial to the health of the human body.
Vaccine Excipient and Media Summary
“Myth: Vaccines are dangerous.”
Fact: Vaccines are inherently dangerous. In an effort to absolve manufacturers of liability for injury, the Supreme Court ruled that vaccines are, in fact, “unavoidably unsafe.”
The current CDC schedule has never been tested for safety and most of the individual vaccines have never been tested in double-blind, inert placebo-controlled studies. We don’t know all that the vaccines do individually, and we certainly don’t know all that they do when injected concomitantly. But we know that there are serious adverse reactions, and that a fraction (less than 1%) of those injured have been “compensated” by the NVICP (National Vaccine Injury Compensation Program).
Vaccine Package Inserts
http://www.vaccinesafety.edu/package_inserts.htm
Vaccine Injury Table
https://www.hrsa.gov/sites/default/files/vaccinecompensation/vaccineinjurytable.pdf
Vaccine Injury Payouts
https://www.hrsa.gov/sites/default/files/hrsa/vaccine-compensation/data/monthly-stats-january-2019.pdf
Less than 1% of Vaccine Adverse Reactions Reported (p 6)
https://www.bmj.com/rapid-response/2011/11/02/underreporting-vaccine-adverse-events
Vaccine Adverse Event Reporting System
https://vaers.hhs.gov/reportevent.html
Supreme Court Statement
http://www.scotusblog.com/case-files/cases/bruesewitz-v-wyeth/
“Vaccines do not cause autism.”
Many replicated studies in mainstream journals show a causal association between vaccines and autism. Each of you should receive a book by J.B. Handley, How to End the Autism Epidemic, accompanied by a letter from Robert F. Kennedy, Jr., shortly. That book contains a plethora of solid evidence, including studies and depositions, to support the argument that vaccines do cause autism. (If you do not receive yours soon, I will personally buy you a copy. Please let me know.)
There is another paper, a meta analysis, being released shortly that contains an even more extensive discussion of the research on vaccines, autism, and epilepsy. It will be shared with each of you, as well.
The only vaccine ever tested in relation to autism was the MMR. Thimerosal, a common vaccine ingredient used as a preservative/adjuvant, was also tested. There are serious questions about the methods used in gathering and reporting that data, but, regardless of the reported outcome of that study, vaccines–plural–have never been tested in connection with autism. Recently, scientists working on other issues with aluminum have discovered that high levels of aluminum are found in the brains of autistics who were examined post mortem.
There is very strong causal association between vaccines and autism. We have access to replicated studies that demonstrate the mechanism, and we have deposed testimony relating to settlements from NVICP for children with autism. Please read How to End the Autism Epidemic for a full discussion on this issue. Also, for a thorough examination of autism diagnosis over the centuries and now, read Denial: How Refusing to Face the Facts about Our Autism Epidemic Hurts Children, Families, and Our Future. And keep your eyes open for the meta analysis from Dr. Bryon Tarbet.
How to End the Autism Epidemic, Chapters 5 and 6, in particular.
Three of Many Studies that Support the Autism/Vaccine Connection Aluminum Hydroxide Injections Lead to Motor Deficits and Motor Neuron Degeneration https://www.ncbi.nlm.nih.gov/pubmed/19740540
Adverse Long term Neurological Outcomes
https://vaccinepapers.org/wp-content/uploads/Shaw-Administration-of-aluminium-to-neonatal-mice-in-vaccine-relevant-amounts-is-associated-with-adverse-long-term-neurological-outcomes.pdf
Aluminum in Brain Tissue in Autism
http://vaccinepapers.org/high-aluminum-content-autistic-brains/
“…fraudulent study written by a discredited doctor…”
There was no study. There was a case series. No conclusions were offered. Just observations and, in a follow-up press conference, a suggestion that the MMR polyvalent vaccine be separated into individual vaccines, until more research could be completed.
Saying something over and over doesn’t make it true. And perpetuating lies does not build credibility.
In addition to autism, there are many other serious adverse reactions to vaccines. Dismissing safety concerns based solely on ignorance of the autism/vaccine discussion, is simplistic, disingenuous, and dangerous.
The NVICP has paid out almost $4 billion for injury compensation since 1986. The injuries on the table linked below are recognized as common adverse reactions to the vaccines they are listed with.
Vaccine Injury Table
https://www.hrsa.gov/sites/default/files/vaccinecompensation/vaccineinjurytable.pdf
That Paper
http://www.rescuepost.com/files/autismfile_us33-wakefield.pdf
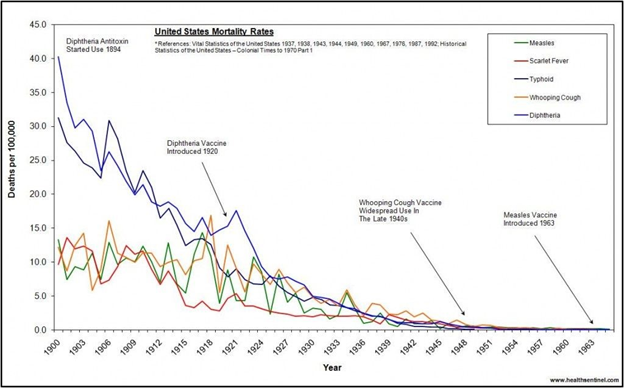
“Myth: Vaccines are Unnecessary” Fact: Mortality for most common childhood infections had already declined significantly before the corresponding vaccines entered the market. The downward trend appears unaffected by vaccine introduction–except where it spikes during vaccination campaigns. Vaccines seem to have decreased the frequency of exposure to common childhood infections, but there is plenty of history indicating that vaccines did not eradicate any infections, and that other factors were the driving force in reducing frequency of exposure and mortality.
Standard infections for which there were no vaccines, like scarlet fever, also decreased dramatically, during the same time period. Correlation doesn’t equal causation.
(Please note the difference between where this graph begins and where the graphs in the “Immunization Education Module” begin. This graph shows the bigger picture.)
There is much to learn about the immune system, the virome, the microbiome, and who knows what else? By injecting substances, the effects of which have not been carefully studied, into our blood streams, we are affecting parts of our immune system that we are just beginning to explore and understand. Casual, simplistic, assumptive statements should not be made by the UDOH or sanctioned by the Utah Legislature. Circumspection is warranted. First do no harm.
I would ask that the UDOH define “necessary.” Do they mean to imply that human life could not exist without vaccines?
“Myth: Giving Vaccines on a delayed schedule or alternate schedule is safer.”
Fact: We do not know. Safety testing of the current CDC schedule has never been done. In fact, as part of the 1986 National Childhood Vaccine Injury Act, which came into play because of injury lawsuits related to the DTP vaccine, HHS was tasked with overseeing the improvement of vaccine safety and reporting to Congress on their progress. They never did it. There is not one report to Congress from HHS on this issue and no documents were produced showing that HHS had followed through on this condition of granting immunity to the vaccine manufacturers.
HHS Stipulated Order
http://icandecide.org/government/ICAN-HHS-Stipulated-Order-July-2018.pdf
Multiple standard vaccines contain aluminum exceeding the EPA recommended safety limit of 25 mcg for an 11 pound baby–a safety limit that applies not to injection into the bloodstream, but to IV, inhalation, or ingestion. Injection is a very different pathway.
Vaccines are tested in clinical studies against a previous version of the vaccine or an adjuvant “placebo” that produces similar reactions. The fact that inert placebos are not used skews the results of the safety trials.
To prove that an alternate schedule is not safer, we would need to compare the different schedules in controlled studies, and a true risk/benefit assessment would need to be done for each, individual vaccine. This has never been done.
We also need a vaccinated vs. completely unvaccinated study, with total health outcomes, in order to determine the safety and efficacy of vaccines and various schedules.
We do not currently know much about vaccine safety, because the testing procedures are wholly inadequate, and there has never been a full scale, independent, inert placebo controlled, vaccinated vs. unvaccinated study.
Vaccine Package Inserts http://www.immunize.org/fda/
Safety Studies are Inadequate
https://www.bmj.com/content/360/bmj.k1378/rr-0
Aluminum and other Toxic Metals (article links to more than a dozen studies)
https://childrenshealthdefense.org/news/aluminum-and-mercury-synergy-a-perfect-storm/
“Vaccine Side Effects: The risks of vaccines are much lower than the risks of the diseases they prevent.”
See point above, including the links.
Where is the research that supports this statement?
The risks listed in the module are the least pernicious risks. The module neglects to mention the more serious adverse reactions listed in vaccine package inserts and safety trial data, such as: Guillain Barre Syndrome, anaphylaxis, encephalitis, encephalopathy, autoimmune diseases, seizure disorders, blindness, death–among many others. If honesty and transparency are the goal, rather than just increasing uptake–regardless of consequences, then these adverse reactions need to be listed in the module, without whitewashing.
“Question 1 of 1”Questions and answers in the module are heavily biased and no reasonable options are offered.
For example: Question: “Why do we need vaccines?”
The assumption is that we need vaccines. Many would disagree with that statement on its face, but all available responses contain false statements, like this one:
Answer option: “We don’t [need vaccines]–those diseases [ referring to common childhood infections] don’t exist anymore.”
We are all aware that, despite vaccines, measles, mumps, and pertussis, at least, are still relatively common. It is irresponsible to over-simplify or manipulate responses this way. Plenty of serious research indicates that vaccines are not the only solution, and may not be the best solution, to safeguarding health. Allow us respond to these questions by sharing real information, instead of having to choose from among inaccurate, pre-written responses.
“What is Community Immunity?” “When enough people are vaccinated contagious diseases will not spread.”
Even in populations where uptake is over 95% we still have outbreaks. Many outbreaks are among those who have been fully vaccinated, including boosters. Some people never develop antibodies when vaccinated. Even if vaccines do produce antibodies, the antibody levels wane. Some people get infections from their vaccines, or from exposure to someone recently vaccinated.
We were told when the first measles vaccine came out that it would be “one and done.” It didn’t work out that way. Now we have multiple boosters for MMR, DTaP, and others. We know, from a study done to determine how antibodies wane in measles, that we can expect measles outbreaks in highly vaccinated populations, due to the lack of natural boosters. As the number of naturally immune individuals goes down, so does herd immunity.
Recent studies show that the flu vaccine doesn’t take effect for a couple of weeks and that it begins to wane–within 28 days. (It makes one wonder when it works.)
Mumps portion of the MMR, specifically, has not reached an efficacious level. Efficacy levels were manipulated by adding rabbit blood and then falsifying the test results, prior to the release of the vaccine. This is currently the subject of a lawsuit. There have been several mumps outbreaks in highly vaccinated populations, with the majority affected having complete vaccine records.
Outbreaks of other “vaccine preventable” infections are also happening, on a fairly regular basis, in highly vaccinated populations.
Chicken Pox Outbreak in Highly Vaccinated School Population
http://pediatrics.aappublications.org/content/113/3/455.short?sso=1&sso_redirect_count=1&nfst atus=401&nftoken=00000000-0000-0000-0000-000000000000&nfstatusdescription=ERROR%3a+No+local+token
Measles Outbreak Among Vaccinated Students
https://www.cdc.gov/mmwr/preview/mmwrhtml/00000359.htm
Measles: Waning Antibodies
https://www.ncbi.nlm.nih.gov/pubmed/16427163
Mumps in Vaccinated Adult Males
https://www.forbes.com/sites/tarahaelle/2014/12/16/nhl-mumps-outbreak-whats-up-with-the-vac cine/amp/
Mumps Lawsuit
http://files.courthousenews.com/2012/06/27/MerckUnsealed.pdf
Pertussis Outbreak Among Vaccinated Preschoolers
https://www.medscape.com/viewarticle/857368
This is just a small sampling. We are happy to provide more references, if anyone would like to see them. High rates of vaccination are not preventing outbreaks.
Mumps Lawsuit
http://files.courthousenews.com/2012/06/27/MerckUnsealed.pdf
Pertussis Outbreak Among Vaccinated Preschoolers https://www.medscape.com/viewarticle/857368
This is just a small sampling. We are happy to provide more references, if anyone would like to see them. High rates of vaccination are not preventing outbreaks.
“Intro to Measles” “At least one out of 1000 people will die, even with the best medical care.”
Where does this statistic come from? Data from just prior to the mass vaccination era showed 3-4 million cases of measles and 400-500 deaths a year. The math isn’t matching up. It seems that these may be third world statistics. It is misleading to use numbers from third world countries to represent the risk of death in this country.
Measles Vaccine History https://www.cdc.gov/measles/about/history.html
“Adults with mumps will occasionally experience serious complications, such as meningitis, deafness, and infertility.”
We would submit that the reason we have large numbers of adults contracting mumps is that the effects of the vaccine, when it works, wane and end up delaying the onset of infection to young adulthood, where consequences can be serious. Mumps is a mild infection, better dealt with in childhood. Vaccines do not produce life-long immunity, and sometimes don’t produce immunity at all.
“Hepatitis A and B” “An infected mother can give her baby the virus during birth.”
The assumption is that every mother is infected with Hepatitis B. Hepatitis B is an STI. If theoretical exposure takes place, what happens when the vaccine is given after exposure? Does the vaccine have time to create antibodies to protect the baby? Where is the research that shows that it is beneficial to vaccinate after exposure?
This slide feels like fear-mongering.
“Diptheria is rare in the United States only because of widespread vaccination against the disease.”
Where are the studies that support this claim? How do we know the vaccines made the difference?
Mortality rates from diptheria were in free-fall starting in 1901 and actually spiked again with the introduction of the vaccine in 1921. (Please see graph in this paper and the handout with graphs.)
“Intro to Pertussis”
Pertussis vaccine is highly ineffective. It also produces asymptomatic carriers, who, by definition, can unknowingly infect others. (It’s kind of like taking Theraflu and then going to work.) Outbreaks of pertussis among highly vaccinated populations are commonplace. Pertussis has been effectively treated with vitamin C therapy. It is serious, but with treatment is beatable, and does not necessarily require hospitalization. In addition, natural immunity protects individuals for a lifetime. Vaccine induced immunity, if there is any, only lasts a few years, hence the need for repeated boosters, and gaps in immunity.
Asymptomatic Carrier Study https://www.ncbi.nlm.nih.gov/pubmed/24277828
“Intro to Tetanus”
Tetanus is not contagious, and, therefore, has no impact on public health and should not be a part of the school vaccine campaign, or part of the module–or part of a polyvalent vaccine.
“Symptoms of Varicella”
I would like to see documentation for the claims of hospitalization and death. Varicella is a mild, short-lived infection. As for concerns about the spread of varicella, varicella is a live virus vaccine. Because of that, the vaccine itself can spread the infection. Use of the vaccine is also implicated in the recent upsurge in shingles, because it breaks the natural “booster” cycle of chicken pox. The UK does not use varicella vaccine for this reason.
Informed consent should be the objective. Giving biased information to increase vaccine uptake is unacceptable.
Varicella Vaccine/UK
https://www.nhs.uk/common-health-questions/childrens-health/why-are-children-in-the-uk-not-va ccinated-against-chickenpox/
“Symptoms of Meningitis”
There is no distinction made in the module between viral and bacterial meningitis. There is no vaccine or treatment for viral meningitis, yet we send everyone out to get the vaccine for bacterial meningitis, leading them to believe they are then protected from meningitis, overall. Again, we do not see any references to the serious adverse reactions from these vaccines in the module. Informed consent requires open access to complete information, and the ability to choose based on complete information.
Pertinent analysis by Robert F. Kennedy Jr., emphasis ours:
“My opposition to new meningitis mandates for every New York State seventh and twelfth grader has nothing to do with autism and everything to do with arithmetic (“Meningitis shot to be rule for schools,” Oct. 28). Meningitis is a rare disease that affect[ed] only 390 people nationally last year. FDA and industry testing show the meningitis vaccine to be unusually low efficacy and high risk. The manufacturers’ inserts predict that 1% to 1.3% of inoculated children will suffer “serious adverse effects.” CDC’s Pink Book forecasts that 0.3% of these will die from the vaccine. Of the 400,000 New York school children inoculated annually, some 4,000 will become ill and nine will die in order to prevent around four people from contracting thedisease. At between $84 and $117 per shot, and with the requirement for a two-shot series, the law is an $80 million annual windfall for vaccine manufacturers at taxpayer expense. This math makes sense only to the pharmaceutical companies and the Albany politicians who have taken their money.”
Pink Book Reference https://www.cdc.gov/vaccines/pubs/pinkbook/mening.html
Information on Meningitis https://www.nvic.org/vaccines-and-diseases/Meningitis/meningitisvaccine.aspxhttps://uhs.umich.edu/meningitis
“Question 1 of 4” “How contagious is measles?”
Level of contagion is not a valid measure of risk. Many mild infections are highly contagious. It is irresponsible to create fear of an infection based simply on how contagious it is. Measles is a mild infection, and has been successfully treated with vitamin A, vitamin C, relatively good nutrition, and rest.
Natural exposure to measles confers lifetime immunity. Vaccination does not. And in some cases vaccination does not even produce an initial immune response.
“How long do people experience symptoms after catching pertussis?” “Up to ten weeks.”
One critical item not mentioned in the module is that individuals who receive the pertussis vaccination are asymptomatic carriers for up to 6 weeks.
Again, once you’ve had natural pertussis, you’re done. You don’t get the same deal with the vaccine, and you run the risk of infecting others (vaccinated and unvaccinated), if you get the vaccine.
Asymptomatic Transmission https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4482312/
“Your Responsibilities/Stay at Home/Make a Plan”
On what basis are we putting healthy vaccine free or selectively vaccinated children under house arrest for 14-26 days, during an outbreak?
We know that vaccinated children can and do contract these common childhood infections, despite boosters. (See links above.) We know that vaccinated individuals can spread these infections, because they are vaccinated.
So why are healthy children being punished? What happens to their grades during that time? What happens to their chances at teams, scholarships, and college entry? What happens to their self-esteem? There is no science-based reason to exclude healthy students from school attendance during outbreaks.
We hesitate to exclude children from school because of behavioral issues due to the emotional trauma, stigma, and danger of precipitating self harm. But it is okay to discriminate against, single out, humiliate, and penalize healthy, diligent students based solely on their vaccination status?
Healthy students are not contributing to the spread of infections. Their educations and futures should not be jeopardized by this unscientific and discriminatory practice.
“Vaccinations Are Simple”
Vaccinations are a medical procedure. Medical procedures have inherent risks, and should be taken seriously, and approached with transparency and full disclosure–at least to the extent that current research allows. Safety and informed consent, not increased uptake, should be the objectives.
________
Thank you for your consideration of our feedback on the UDOH “Immunization Education Module.” This feedback has been submitted on behalf of Your Health Freedom, a group of Utah parents who favor informed consent in all medical interventions, and the Utah Eagle Forum.
If you have questions, comments, or concerns please contact Kristen Chevrier at [email protected].
We are happy to meet with both law and rule makers to discuss issues surrounding vaccine research and policy.